
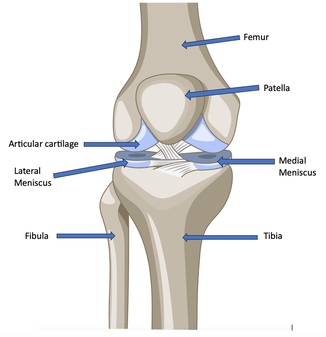
A new study in the New England Journal of Medicine found that a common meniscus surgery does no better than a fake operation, suggesting that thousands of people may be undergoing unnecessary surgery every year. A New York Times article about the study says:
Arthroscopic surgery on the meniscus is the most common orthopedic procedure in the United States, performed, the study said, about 700,000 times a year at an estimated cost of $4 billion.

The study had half the people undergo normal arthroscopic partial meniscectomy and the other half received anesthesia and incisions but no real surgery. A year later most patients in both groups said their knees felt better and said they would choose the same procedure again, even if it was the sham surgery.
“Those who do research have been gradually showing that this popular operation is not of very much value,” said Dr. David Felson, a professor of medicine and epidemiology at Boston University. This study “provides information beautifully about whether the surgery that the orthopedist thinks he or she is doing is accomplishing anything. I think often the answer is no.”
This isn't the first time a study has shown knee surgery might not very effective or more effective than other less invasive treatments.
The new research builds on a groundbreaking 2002 Texas study, showing that patients receiving arthroscopy for knee osteoarthritis fared no better than those receiving sham surgery. A 2008 Canadian study found that patients undergoing surgery for knee arthritis did no better than those having physical therapy and taking medication. Now many surgeons have stopped operating on patients with only knee arthritis.
Earlier this year, a study at seven American hospitals found that patients with meniscal tears and osteoarthritis did not experience greater improvement with surgery than those receiving physical therapy, although after six months, one-third of the physical therapy group sought surgery. (Their surgical results were not reported.)
The New York Times article interviewed Dr. Kenneth Fine, an orthopedic surgeon, and this is what he says:
“Take 100 people with knee pain; a very high percentage have a meniscal tear,” said Dr. Kenneth Fine, an orthopedic surgeon who also teaches at George Washington University. “People love concreteness: ‘There’s a tear, you know. You have to take care of the tear.’ I tell them, ‘No. 1, I’m not so sure the meniscal tear is causing your pain, and No. 2, even if it is, I’m not sure the surgery’s going to take care of it.”
Dr. Fine added: “Yours truly has a meniscal tear. It just causes pain. I’m not having any mechanical symptoms; my knees are not locking. So I’m not going to let anybody operate.”
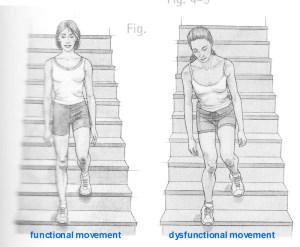
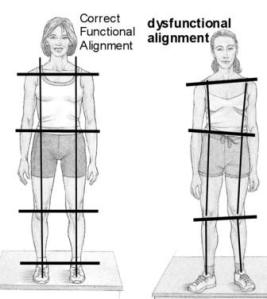
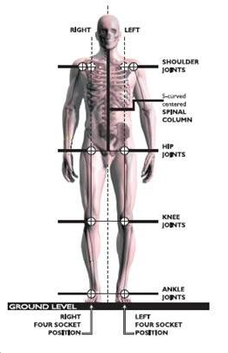
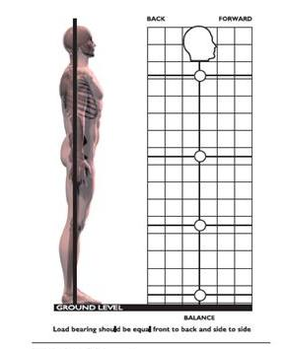
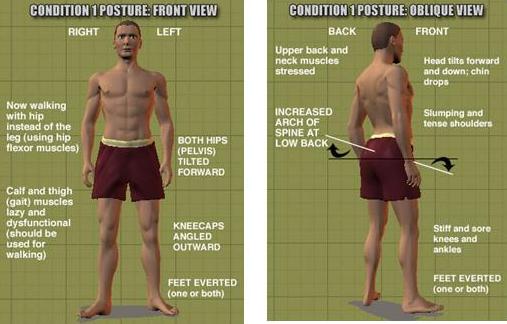
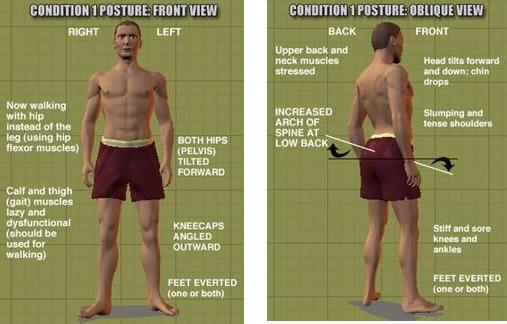
What if our medical system could move away from trying to find a broken piece and surgically repair it, and start looking at the entire body to find the cause of the problem?
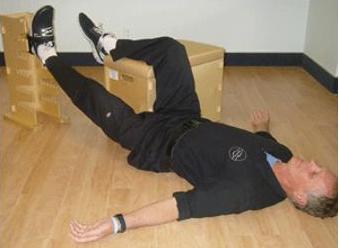
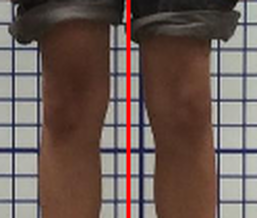
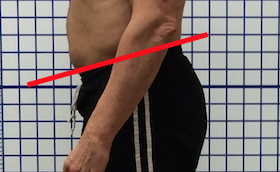
I've helped many clients with meniscal tears and other problems who were told they need surgery and by correcting their muscular imbalances, restoring proper biomechanical movement patterns and improving their posture they have been able to avoid surgery and return to a pain free and active life.
Here is what one client had to say:
I've helped many clients with meniscal tears and other problems who were told they need surgery and by correcting their muscular imbalances, restoring proper biomechanical movement patterns and improving their posture they have been able to avoid surgery and return to a pain free and active life.
Here is what one client had to say:
I could not straighten my injured left leg because of a "flap" on the torn meniscus. My doctor told me I needed surgery to correct the flap. Unbelievably, six visits later the pain was completely gone and I could straighten the leg my doctor told me would be impossible without surgery. I have become an advocate for Matt Whitehead and Oregon Exercise Therapy (OET). Do yourself a favor; check out OET before you consider surgery. Some simple exercises might help you avoid the cost and recovery time of medical intervention.
Part of the problem could also be financial and the way the referral system works, as Dr. Fine said:
He (Dr. Fine) likened the recent studies to attempts to educate people that “it’s not really good to take antibiotics for the common cold. There’s a lot of pressure to operate. Financial, obviously. But also, if a primary care doctor keeps sending me patients who are complaining of knee pain and I keep not operating on them, then the primary care doctor is going to stop sending me patients.”
If you are looking for a way to help yourself become pain free and be able to return to a physically active life without limitations, contact me today set up a free posture evaluation. You can do your consultation on Zoom from anywhere in the world from the comfort of your home or office.
Related articles:
Patellofemoral pain syndrome and your posture
Knee joint osteoarthritis
Preventing ACL injuries
Patellofemoral pain syndrome and your posture
Knee joint osteoarthritis
Preventing ACL injuries
- Arthroscopic Partial Meniscectomy versus Sham Surgery for a Degenerative Meniscal TearRaine Sihvonen, M.D., Mika Paavola, M.D., Ph.D., Antti Malmivaara, M.D., Ph.D., Ari Itälä, M.D., Ph.D., Antti Joukainen, M.D., Ph.D., Heikki Nurmi, M.D., Juha Kalske, M.D., and Teppo L.N. Järvinen, M.D., Ph.D. for the Finnish Degenerative Meniscal Lesion Study (FIDELITY) Group N Engl J Med 2013; 369:2515-2524December 26, 2013DOI: 10.1056/NEJMoa1305189 http://www.nejm.org/doi/full/10.1056/NEJMoa1305189
- A Controlled Trial of Arthroscopic Surgery for Osteoarthritis of the KneeJ. Bruce Moseley, M.D., Kimberly O'Malley, Ph.D., Nancy J. Petersen, Ph.D., Terri J. Menke, Ph.D., Baruch A. Brody, Ph.D., David H. Kuykendall, Ph.D., John C. Hollingsworth, Dr.P.H., Carol M. Ashton, M.D., M.P.H., and Nelda P. Wray, M.D., M.P.H. N Engl J Med 2002; 347:81-88 July 11, 2002DOI: 10.1056/NEJMoa013259 http://www.nejm.org/doi/full/10.1056/NEJMoa013259
- A Randomized Trial of Arthroscopic Surgery for Osteoarthritis of the KneeAlexandra Kirkley, M.D., Trevor B. Birmingham, Ph.D., Robert B. Litchfield, M.D., J. Robert Giffin, M.D., Kevin R. Willits, M.D., Cindy J. Wong, M.Sc., Brian G. Feagan, M.D., Allan Donner, Ph.D., Sharon H. Griffin, C.S.S., Linda M. D'Ascanio, B.Sc.N., Janet E. Pope, M.D., and Peter J. Fowler, M.D. N Engl J Med 2008; 359:1097-1107September 11, 2008DOI: 10.1056/NEJMoa0708333 http://www.nejm.org/doi/full/10.1056/NEJMoa0708333
- Common Knee Surgery Does Very Little for Some, Study Suggests By PAM BELLUCKPublished: December 25, 2013 http://www.nytimes.com/2013/12/26/health/common-knee-surgery-does-very-little-for-some-study-suggests.html?emc=eta1&_r=1&









 RSS Feed
RSS Feed