
Patellofemoral pain syndrome (PFPS) or "runner's knee" is characterized by pain and discomfort originating from the contact of the posterior surface of the patella (kneecap) and the femur. Patellofemoral pain syndrome usually involves acute or chronic lateral dislocation of the patella. This means the patella is sliding laterally (to the outside) in and out of its groove. This causes thinning and softening of the articular cartilage on the underside of the patella (chondromalacia) and/or on the medial or lateral femoral condyles.
The lateral dislocation is usually blamed on a weak vastus medialis muscle and overly strong vastus lateralis muscle and typical exercise therapy or physical therapy involves quad strengthening exercises that attempt to correct this imbalance. I agree that this imbalance is often present, but I rarely believe it is the cause of the problem, but rather a symptom of, or compensation for, a much bigger problem.
The lateral dislocation is usually blamed on a weak vastus medialis muscle and overly strong vastus lateralis muscle and typical exercise therapy or physical therapy involves quad strengthening exercises that attempt to correct this imbalance. I agree that this imbalance is often present, but I rarely believe it is the cause of the problem, but rather a symptom of, or compensation for, a much bigger problem.

Many scientific studies have linked hip muscle imbalances to patellofemoral pain. To understand how weak hip muscles can cause patellofemoral knee pain, lets look at what these muscles do and how weakness affects posture, joint mechanics, and gait.
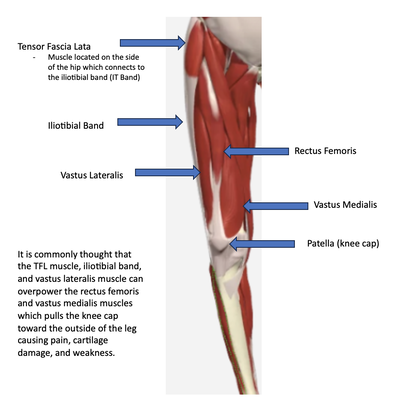
The image and accompanying text below expand the "quad imbalance view" to include a weak rectus femuris, a strong tensor fascia lata (TFL) and a tight iliotibial (IT) band that all play a role in the faulty patellar tracking. The TFL is a strong hip flexor that also abducts and internally rotates the femur and externally rotates the tibia. The TFL via the IT band can thus create internal femur rotation while at the same time creating external tibial rotation and, via the fascia that connects the IT band to the lateral side of the patella, will have the effect of pulling the patella in and out of its groove as the hip and knee flexes and extends. Physical therapists, exercise specialists, and personal trainers who look at this larger picture will include stretching for the IT band and TFL muscle along with the quad strengthening exercises mentioned previously.
The image and accompanying text below expand the "quad imbalance view" to include a weak rectus femuris, a strong tensor fascia lata (TFL) and a tight iliotibial (IT) band that all play a role in the faulty patellar tracking. The TFL is a strong hip flexor that also abducts and internally rotates the femur and externally rotates the tibia. The TFL via the IT band can thus create internal femur rotation while at the same time creating external tibial rotation and, via the fascia that connects the IT band to the lateral side of the patella, will have the effect of pulling the patella in and out of its groove as the hip and knee flexes and extends. Physical therapists, exercise specialists, and personal trainers who look at this larger picture will include stretching for the IT band and TFL muscle along with the quad strengthening exercises mentioned previously.
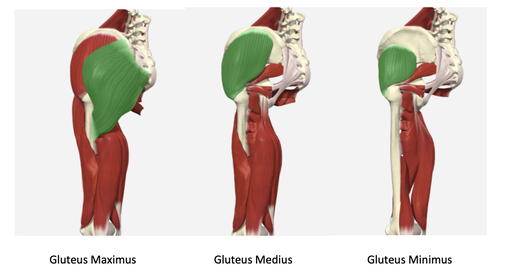
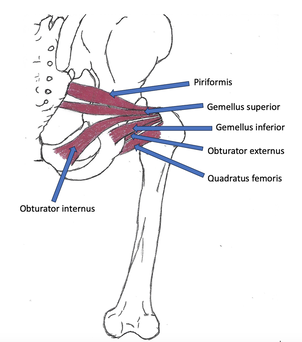
Research is showing that this approach is still missing a very important component of PFPS and physical therapy, exercise therapy, and rehabilitation should be adapted to include the latest findings. Three high quality studies have come out in 2013 that link hip muscle imbalances to patellofemoral pain, most pointing to weak hip abductor and hip external rotator muscles especially weak gluteus medius muscles. A review of 47 published studies in the British Journal of Sports Medicine examined factors causing PFPS and showed that decreased muscle strength in hip abduction and hip external rotation are important facts associated with PFPS. This means the gluteal muscles (gluteus maximus, gluteus medius, gluteus minimus), which help with hip abduction and external rotation, and the deep six (piriformis, gemellus superior, obturator internus, gemellus inferior, quadratus femoris, and obturator externus), which do lateral or external hip rotation and help with hip abduction, play a really important role in controlling femur position which dictates patellar position and tracking.
Now good exercise therapy will take into account all these muscles groups and their respective strength or weakness when developing an exercise routine to combat patellar tracking issues and patellofemural pain syndrome. But could there possibly be anything else involved in dysfunctional movement patterns that create PFPS?
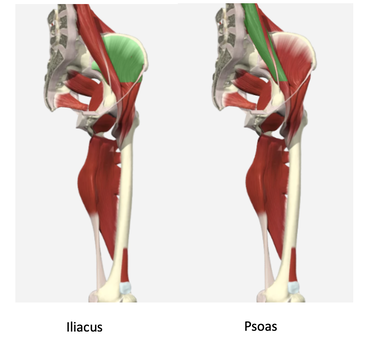
What about the iliacus and psoas muscles?
What about the iliacus and psoas muscles?
|
The psoas and iliacus both play a role in controlling excessive internal rotation of the femur just like the deep gluteal muscles and they can play a role in stabilizing the pelvis just like the abductor group, not allowing a hip drop during gait, seen as a Trendelenburg Sign.
​A Trendelenburg Sign, excessive internal rotation of the femur, or valgus or varus stress at the knee are all signs of likely weakness of ipsilateral psoas and iliacus, contralateral hip abductors, and contralateral external femur rotators. |
The psoas and iliacus are the most powerful hip flexors and when they are weak or dysfunctional, other muscles have to take over there role. What muscles start to take over? The TFL via the IT band and the rectus femoris. With psoas weakness the femur will internally rotate which puts the TFL and IT band into a more forward position to take over as the primary hip flexor. This overuse will create tightness along the TFL and IT band. The rectus femoris and TFL via the IT band, as they are overworked, creates excessive force pulling the patella laterally during gait creating the wear and tear on the surrounding cartilage.
While walking, climbing stairs, or running your feet and knees should point straight ahead and your hips/pelvis should remain almost level. Weakness in the above mentioned muscles allows excessive movement in the transverse and frontal planes which creates forces on the knee and patella that can pull it out of its groove causing PFPS.
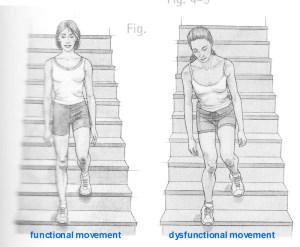
How does someone with weak hip muscles move from point A to point B? By compensating for the weak muscles and creating compensatory movement throughout the entire body as can be seen below. The woman on the left is showing proper movement patters. The woman on the right is showing dysfunctional movement caused by weak and imbalanced hip musculature which is creating compensatory movements throughout her body. Those compensatory movements create muscle imbalances up and down the entire body. Images below from Pete Egoscue's book Pain Free for Women.
While walking, climbing stairs, or running your feet and knees should point straight ahead and your hips/pelvis should remain almost level. Weakness in the above mentioned muscles allows excessive movement in the transverse and frontal planes which creates forces on the knee and patella that can pull it out of its groove causing PFPS.
How does someone with weak hip muscles move from point A to point B? By compensating for the weak muscles and creating compensatory movement throughout the entire body as can be seen below. The woman on the left is showing proper movement patters. The woman on the right is showing dysfunctional movement caused by weak and imbalanced hip musculature which is creating compensatory movements throughout her body. Those compensatory movements create muscle imbalances up and down the entire body. Images below from Pete Egoscue's book Pain Free for Women.
Movement is posture in motion. We can look at static standing posture to understand why we see what we do during movement. The static standing posture of the two women above is shown below from Pain Free for Women by Pete Egoscue:
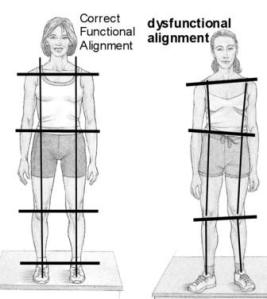
The woman on the left shows proper posture with correct alignment of all eight of her major load joints - ankles, knees, hips, and shoulders. They are all vertically and horizontally aligned. This means she has good muscular balance throughout her body. This allows her to walk, run, squat, lift, and climb stairs without losing proper bone alignment and joint movement patterns.
The woman on the right shows many postural imbalances: dropped right shoulder, right lateral head tilt, torso offset to left, right elevated pelvis/hip, valgus knee position, externally rotated right femur, everted feet right more than left. If all these imbalances are not corrected, strengthening the vastus medialis and gluteus medius and stretching the IT band will have very little if any long term benefit. The body is a unit and when treated as one patallofemoral pain syndrome and any other musculoskeletal pain can become a thing of the past.
The woman on the right shows many postural imbalances: dropped right shoulder, right lateral head tilt, torso offset to left, right elevated pelvis/hip, valgus knee position, externally rotated right femur, everted feet right more than left. If all these imbalances are not corrected, strengthening the vastus medialis and gluteus medius and stretching the IT band will have very little if any long term benefit. The body is a unit and when treated as one patallofemoral pain syndrome and any other musculoskeletal pain can become a thing of the past.
- Lankhorst NE, Bierma-Zeinstra, SMA, and van Middelkoop, M. Factors associated with patellofemoral pain syndrome: a systematic review. Br J Sports Med. 2013;47:193–206.
- Barton CJ, Lack, S, Malliaras, P, and Morrissey, D. Gluteal muscle activity and patellofemoral pain syndrome: a systematic review. Br J Sports Med. 2013; 47:207–214.
- Selkowitz, DM, Beneck, GJ, and Powers CM. Which Exercises Target the Gluteal Muscles While Minimizing Activation of the Tensor Fascia Lata? Electromyographic Assessment Using Fine-Wire Electrodes. J Orthop Sports Phys Ther. 2013; 43(2):54-64.
 RSS Feed
RSS Feed